Key Considerations for Reaching Adolescent Girls with HPV Vaccine from JSI’s Experience Supporting Roll-out in Multiple Countries
April 23rd, 2019 | viewpoint
Gavi, the Vaccine Alliance, has an ambitious target of administering the human papillomavirus (HPV) vaccine to 40 million girls ages 9–14 by 2020. JSI has been supporting Ministries of Health in eight countries as they plan for and introduce this life-saving vaccine, and in doing so has learned a lot about how to reach adolescent girls.
While many Gavi-supported countries have introduced new vaccines—pentavalent, rotavirus, PCV, and others—in the past decade, the introduction of the HPV vaccine requires different approaches. Because it targets pre-adolescent/adolescent girls (and not the usual children 0–5 years old), new strategies are required to reach this population. This includes linking with other cancer-prevention and adolescent health initiatives and services, communicating the importance of HPV vaccination, and coordinating with partners that have not previously been involved with the Expanded Program on Immunization (EPI).
The successful rollout and uptake of HPV vaccine requires investments over several years, and a detailed focus during preparation and particularly post-launch to ensure sustainability and future coverage with each year’s cohort. Four major considerations emerged from JSI’s recent support in Zimbabwe, Tanzania, and Malawi:
Communicating with communities, parents, and the girls being vaccinated
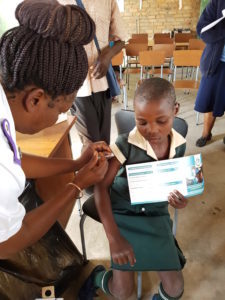
Understanding the audience is always necessary when developing marketing materials for health services. Different from infant vaccines, the HPV vaccine is provided to people who are old enough to ask questions and make decisions about their own bodies and health care. As such, messages must be targeted directly to the girls in addition to their parents or caregivers. In Tanzania, JSI has helped the MOH develop and pretest information, education, and communications materials, including television and radio sports targeted to girls, their parents, and the community as a whole.
A mother (doing her daughter’s hair) is surprised when her husband returns home earlier than normal. The husband responds that he has just heard the news on the radio about the introduction of a vaccine to prevent cervical cancer. He continues that he heard that in order for girls to be protected, they have to get the second dose of the vaccine six months after the first dose. Their daughter then intervenes by saying that it is true and has been six months since she received the first dose. The father tells his daughter to go and get ready so that he can take her to the health facility to get the second dose.
In addition to targeting communication to girls and their parents, it’s important to work with and tailor messages to community and religious leaders, local nongovernmental and civil society organizations, and the media. A proactive approach to ensure that information is accurately and efficiently conveyed to various community stakeholders can prevent the spread of misinformation and stigma. In Malawi, for example, JSI participated in WhatsApp and Facebook groups with district managers to dispel rumors and answer questions about the vaccine.

Working with ministries of education, schools, and teachers
Another effective way to reach pre- and adolescent girls is through schools, especially in countries that have higher school enrollment. In Zimbabwe and Malawi, health workers are working with teachers to develop lists of eligible girls and have traveled to the schools to vaccinate them. By providing the vaccine in schools, health workers reach a large number of girls at one time and can track those who need their second dose. Providing the two doses of HPV to girls at ages when they are still likely to be in school is an effective way to reach a larger proportion of this population. Challenges arise when girls do drop out of or switch schools between the first and second doses. In Zimbabwe, officials are working with schools to keep their lists updated so that such girls can be tracked and given their second dose.

Preventing cancer
Unlike measles and polio (two other vaccine-preventable diseases that are known in communities and part of child vaccination schedules), the HPV vaccine protects against cancer that generally affects women decades after they are first exposed to HPV. Further, cervical cancer is not well understood (or feared) because it is not visible and is less likely to be perceived as a threat. It is therefore important for communication strategies to include an explanation of cervical cancer and the benefits of HPV vaccine for cancer prevention. Together, EPI officials, other departments within the ministry of health, local cancer-prevention and gynecological organizations, and partners must ensure that the vaccine is integrated with other disease screening and treatment activities. JSI highlighted the importance of engaging with new stakeholders during its support of the demonstration project in Madagascar.
Determining and analyzing target populations and data
Coverage is a key indicator for measuring and monitoring immunization achievements. For HPV in particular, however, coverage can be especially difficult to calculate because the total population of adolescent girls is often unknown. Countries have used multiple data sources, including census and school registers, to estimate their target populations. In Zimbabwe, the ministries of health and education completed a mapping exercise with support from civil society organizations and community leaders to identify all eligible girls. After the first round of vaccinations, data discrepancies were addressed at the district level through a detailed verification exercise.
Along with understanding the target population, it is also important to track the number of eligible girls who have received the vaccine to verify and validate coverage. Out-of-school girls may be missed if outreach is insufficient or if their numbers have not been calculated accurately. In other cases, girls outside the eligible age range have been vaccinated (for example, due to confusion on calculating the exact target age). This can result in coverage being higher than anticipated, making it difficult to know exactly how many of the originally eligible girls have been missed. It also can inadvertently result in vaccine stockouts because more girls are vaccinated than had been planned. Clear communication with health workers and others supporting vaccination roll-out on who is eligible will help to ensure that girls are not left out or missed. It is also imperative to have updated name-based registers and vaccination cards to track who has been vaccinated and the doses received.

With vaccination linked to reduced disease incidence and transmission, further cross-country learning, use of resources, and opportunities to continue roll-out of HPV vaccine as part of cervical cancer elimination are increasingly recommended, particularly in lower-income countries. JSI is currently supporting Kenya and Cameroon’s planned 2019 HPV vaccine introductions and continues to support Malawi, Zimbabwe, and Tanzania. We also look forward to working with ministries of health and partners to share lessons on improving and maintaining coverage rates in countries that have already introduced the vaccine.
Written by Kristin Krudwig
We strive to build lasting relationships to produce better health outcomes for all.




