Data-Powered Decisions: How an Ethiopian Health Center Improved Antenatal Care
December 30th, 2019 | story
In Tigray, Ethiopia, Tsadekan, who is seven months pregnant with her fifth child, is at the Hawelti Health Center for what should be her third antenatal care (ANC) visit after skipping her second appointment. “I didn’t know that I needed to come back. I thought I only come back [to the health center] if I felt unwell,” says Tsadekan. She was not alone in her assumption. In fact, mothers missing ANC visits was recently a top problem for the Hawelti Health Center.
Finding the Problem
The health center established a quality improvement team (QIT) to prioritize problems, analyze their root causes, and develop and implement interventions to overcome them through regular performance monitoring meetings. Prioritization involves a process of ranking problems by their severity, based on a grading system that is approved by the Ethiopian Ministry of Health. Problems with the highest marks are given top priority.
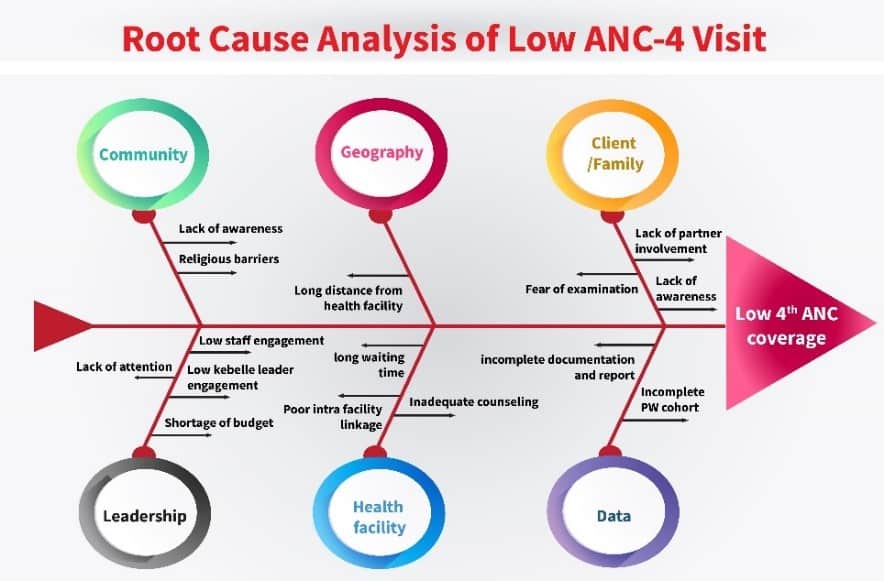
During a January 2019 performance monitoring meeting, the QIT identified multiple underperforming programs. According to the prioritization matrix, low turnout for the fourth ANC visit (ANC4), which is supposed to occur between the 37th and 40th weeks of pregnancy, was an urgent problem. The QIT conducted a root cause analysis to determine the underlying reasons and mapped the causes under categories such as leadership, community, health facility, geography, data, and family. The QIT prioritized the root causes that could have the greatest impact. Among the causal factors were an inadequately functioning pregnant women cohort system, low health extension worker (HEW) engagement, low midwife participation, lack of partner involvement, and poor intra-facility referral linkage.
Implementing Solutions
Next, the QIT made a list of practical solutions and started implementing them. With the help of midwives, they created a list of defaulters (pregnant women who missed ANC appointments) from the pregnant women registry. Each Friday, an HEW supervisor gave a list of defaulters and their relevant information to HEWs. Over the weekend, the HEWs, in collaboration with the head of the women’s development army, found and talked to the women and made ANC appointments for them at the health center for the following week.
The second promising intervention was strengthening intra-facility referral linkages. The QIT found that many women who tested positive for pregnancy after visiting the health center’s outpatient department were not referred to the maternal and child health (MCH) department: in the first three months of 2019, 98 of 143 women who visited the health center for pregnancy tests were confirmed pregnant. But only 60 of them started ANC services.
“This was a shocking revelation. We are supposed to have them continue attending the service,” says Daniel Meressa, director of the health center, who was dismayed at the finding. To remedy the issue, the health center instructed staff who conduct pregnancy tests to automatically link women who test positive to the MCH department for antenatal care. A few months following the decision, the health center’s QIT reviewed the data from the interventions. ANC4 completion was at 52 percent when the intervention started. By June 2019, the completion rate jumped to 60 percent.
“This result was not enough. But it indicates what we can do if we put our act together,” says Daniel. While the increase in completion rate was modest, it was enough to boost the health center staff’s morale. In July 2019, the second phase of the intervention began, aiming to increase ANC4 visits to 85 percent before the end of June 2020. In addition to strengthening the aforementioned interventions, the QIT recommended focusing on ways to identify pregnant women earlier by enhancing home visits, conducting family conversations, holding campaigns, and streamlining ANC services in the routine work of the kebele administrators.
Accordingly, kebele administration mobilized communities to pave roads to health facilities. HEWs conducted several home-to-home visits and talked with 49 families. It was one such family conversation that led Tsadekan back to receive ANC services after she missed her second appointment. “I lost my third child three days after he was born. I didn’t attend ANC during his pregnancy. Now, I began to think if his death was related to any of this,” she confides.
Long distances to the health center in addition to long wait times contributed to the low turnout for ANC4 service, as did the fact that Hawelti serves a large population and is only supported by two health posts. The QIT expanded ANC services at the health posts, which are closer to many women’s homes, sending midwives to the health posts with the necessary equipment to provide ANC services to 10–15 women a day.

Further, the health center extended tracing to all ANC visits, not just ANC4. HEWs, in close collaboration with head of women’s development army and the kebele administrator, make sure that pregnant women are linked from one ANC visit to the next. “Although this is bit too much with limited human resources and number of facilities, we needed to do this. We could not find another easy way of coming out of this,” says Daniel.
Improving Health Outcomes
By the end of November 2019, the percentage of women who completed ANC4 visits had grown from 60 percent in June 2019 to 79 percent. More importantly, 86 percent of the women who test positive for pregnancy at the health center are linked to and start attending ANC services, a substantial increase from before the health center implemented these changes.
Ultimately, these efforts are helping more women give birth at the health facility, where they are attended by skilled professionals; such deliveries rose from 67 percent in June to 88.5 percent in November. The Hawelti Health Center still has progress to make, but thanks to the diligence of its QIT and staff, ANC visits and skilled deliveries are on the rise, proving that having a clear process to routinely review and use data to inform decision-making can improve maternal and child health care service use and in turn, health outcomes.
The Ethiopia Data Use Partnership (DUP) is a collaborative endeavor of the Ethiopian Ministry of Health to improve the collection and use of high quality routine health information, leading to better primary health and nutrition services at all levels of the health system. DUP is funded by the Bill & Melinda Gates Foundation and the Doris Duke Charitable Foundation and includes partners, JSI Research & Training Institute, Inc. and the University of Gondar.
We strive to build lasting relationships to produce better health outcomes for all.




